Overview
 A bunion is a very common foot deformity that develops over the first metatarsal phalageal joint of the big toe of the foot. The joint that joins the big toe to the foot is called the first MTP joint. When it becomes prominent and the big toe starts to become crooked this is known as a bunion. The term referring to deformity of the big toe as it becomes crooked is called Hallux Valgus. It is the bump itself that is known as the bunion. When it gets red and swollen over the bunion because it gets sore this is usually due to an inflamed soft tissue over the underlying bone.
A bunion is a very common foot deformity that develops over the first metatarsal phalageal joint of the big toe of the foot. The joint that joins the big toe to the foot is called the first MTP joint. When it becomes prominent and the big toe starts to become crooked this is known as a bunion. The term referring to deformity of the big toe as it becomes crooked is called Hallux Valgus. It is the bump itself that is known as the bunion. When it gets red and swollen over the bunion because it gets sore this is usually due to an inflamed soft tissue over the underlying bone.
Causes
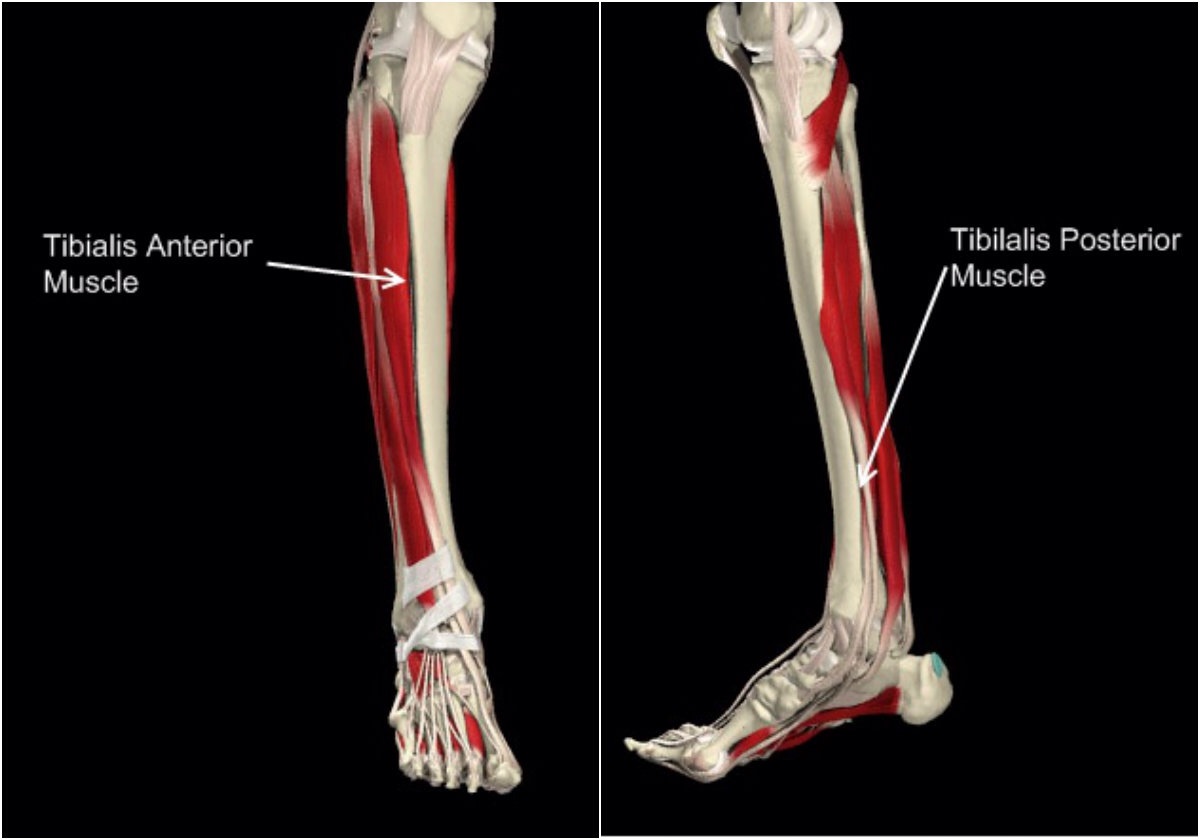
Causes of bunions and risk factors for bunions include a family tendency to bunions may make them more likely to develop. Arthritis of the foot, if it affects walking, it can make bunions more likely to develop. Neuromuscular problems, such as cerebral palsy. Biomechanical factors, such as low arches, flat feet and hypermobile joints, can increase the risk. Wearing shoes that are too tight, too narrow and with pointed toes will exacerbate symptoms if bunions are present. Wearing high heels will also exacerbate existing bunions. Women are more prone to bunions than men.
Symptoms
Symptoms include pain in and around the ball of the big toe, usually from the bone rubbing too much against the shoe. You may be unable to wear certain types of shoes due to the shape of the forefoot. The big toe appears to be bent inwards towards and in come cases over the inside toe.
Diagnosis
Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment.
Non Surgical Treatment
Bunion treatment should always start with changing footwear to relieve symptoms and to prevent the bunion from progressing. Shoes with a wide toe-box, minimal slope, and good arch support can help relieve the bunion pain. Some people find that ice application and anti-inflammatory medications can help relieve the inflammation around the bunion.
Surgical Treatment
If other treatments don?t help and your bunion is very painful, you may be referred to an orthopaedic or a podiatric surgeon for assessment. There are over 130 different operations that can be carried out to treat bunions. The simplest operations are called bunionectomies. The majority of the operations aim to correct the alignment of your big toe. This will narrow your foot and straighten out your big toe joint as much as possible. An operation won?t return your foot back to normal, but most people find that surgery reduces their symptoms and improves the shape of their foot. The operation your surgeon will advise you to have will depend on how severe your bunion is and whether or not you have arthritis.
A bunion is a very common foot deformity that develops over the first metatarsal phalageal joint of the big toe of the foot. The joint that joins the big toe to the foot is called the first MTP joint. When it becomes prominent and the big toe starts to become crooked this is known as a bunion. The term referring to deformity of the big toe as it becomes crooked is called Hallux Valgus. It is the bump itself that is known as the bunion. When it gets red and swollen over the bunion because it gets sore this is usually due to an inflamed soft tissue over the underlying bone.Causes
Causes of bunions and risk factors for bunions include a family tendency to bunions may make them more likely to develop. Arthritis of the foot, if it affects walking, it can make bunions more likely to develop. Neuromuscular problems, such as cerebral palsy. Biomechanical factors, such as low arches, flat feet and hypermobile joints, can increase the risk. Wearing shoes that are too tight, too narrow and with pointed toes will exacerbate symptoms if bunions are present. Wearing high heels will also exacerbate existing bunions. Women are more prone to bunions than men.
Symptoms
Symptoms include pain in and around the ball of the big toe, usually from the bone rubbing too much against the shoe. You may be unable to wear certain types of shoes due to the shape of the forefoot. The big toe appears to be bent inwards towards and in come cases over the inside toe.
Diagnosis
Diagnosis begins with a careful history and physical examination by your doctor. This will usually include a discussion about shoe wear and the importance of shoes in the development and treatment of the condition. X-rays will probably be suggested. This allows your doctor to measure several important angles made by the bones of the feet to help determine the appropriate treatment.
Non Surgical Treatment
Bunion treatment should always start with changing footwear to relieve symptoms and to prevent the bunion from progressing. Shoes with a wide toe-box, minimal slope, and good arch support can help relieve the bunion pain. Some people find that ice application and anti-inflammatory medications can help relieve the inflammation around the bunion.
Surgical Treatment
If other treatments don?t help and your bunion is very painful, you may be referred to an orthopaedic or a podiatric surgeon for assessment. There are over 130 different operations that can be carried out to treat bunions. The simplest operations are called bunionectomies. The majority of the operations aim to correct the alignment of your big toe. This will narrow your foot and straighten out your big toe joint as much as possible. An operation won?t return your foot back to normal, but most people find that surgery reduces their symptoms and improves the shape of their foot. The operation your surgeon will advise you to have will depend on how severe your bunion is and whether or not you have arthritis.




 An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears. Causes The most common cause of a ruptured Achilles' tendon is when too much stress is placed through the tendon, particularly when pushing off with the foot. This may happen when playing sports such as football, basketball or tennis where the foot is dorsiflexed or pushed into an upward position during a fall. If the Achilles' tendon is weak, it is prone to rupture. Various factors can cause weakness, including corticosteroid medication and injections, certain diseases caused by hormone imbalance and tendonitis. Old age can also increase the risk of Achilles' tendon rupture. Symptoms Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel, an inability to bend your foot downward or "push off" the injured leg when you walk, an inability to stand on your toes on the injured leg, a popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward. Diagnosis A typical history as detailed above together with positive clinical examination usually will clinch the diagnosis. In an acute rupture, one can usually feel the gap in the tendon from the rupture. There may be swelling or bruising around the ankle and foot of the injured leg. With the patient lying on the tummy (prone position) with the knee flexed, the examiner should see the ankle and foot flex downwards (plantarward) when squeezing the calf muscles. If there is no movement in the ankle and foot on squeezing the calf muscle, this implies that the calf muscle is no longer attached to the heel bone due to a complete Achilles tendon rupture. Non Surgical Treatment The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex?, Advil?, Motrin?, Naprosyn?. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.
An Achilles tendon rupture, or tear, is a common condition. This typically occurs in the unconditioned individual who sustains the rupture while playing sports, or perhaps, from tripping. There is a vigorous contraction of the muscle and the tendon tears. Causes The most common cause of a ruptured Achilles' tendon is when too much stress is placed through the tendon, particularly when pushing off with the foot. This may happen when playing sports such as football, basketball or tennis where the foot is dorsiflexed or pushed into an upward position during a fall. If the Achilles' tendon is weak, it is prone to rupture. Various factors can cause weakness, including corticosteroid medication and injections, certain diseases caused by hormone imbalance and tendonitis. Old age can also increase the risk of Achilles' tendon rupture. Symptoms Although it's possible to have no signs or symptoms with an Achilles tendon rupture, most people experience pain, possibly severe, and swelling near your heel, an inability to bend your foot downward or "push off" the injured leg when you walk, an inability to stand on your toes on the injured leg, a popping or snapping sound when the injury occurs. Seek medical advice immediately if you feel a pop or snap in your heel, especially if you can't walk properly afterward. Diagnosis A typical history as detailed above together with positive clinical examination usually will clinch the diagnosis. In an acute rupture, one can usually feel the gap in the tendon from the rupture. There may be swelling or bruising around the ankle and foot of the injured leg. With the patient lying on the tummy (prone position) with the knee flexed, the examiner should see the ankle and foot flex downwards (plantarward) when squeezing the calf muscles. If there is no movement in the ankle and foot on squeezing the calf muscle, this implies that the calf muscle is no longer attached to the heel bone due to a complete Achilles tendon rupture. Non Surgical Treatment The treatments of Achilles tendonitis include resting the painful Achilles tendon will allow the inflammation to subside and allow for healing. A period of rest after the onset of symptoms is important in controlling Achilles tendonitis. In patients who have more significant symptoms, a period of immobilization can help. Either a removable walking boot or a cast can allow the inflamed tendon to cool down quickly. A heel wedge can be inserted into the shoe to minimize the stress on the Achilles tendon. These can be placed in both athletic and work shoes. Applying ice to the area of inflammation can help stimulate blood flow to the area and relieve the pain associated with inflammation. Apply ice several times a day, including after exercise. The pain and swelling most commonly associated with Achilles tendonitis can be improved with non-steroidal, anti-inflammatory medications (NSAIDs) which include Celebrex?, Advil?, Motrin?, Naprosyn?. Be sure to consult your physician before starting any medications. Physical therapists can help formulate a stretching and rehabilitation program to improve flexibility of the Achilles tendon. Cortisone injections should not be used for Achilles tendonitis. Studies have shown an increased incidence of Achilles tendon rupture after cortisone injections.  Surgical Treatment Unlike other diseases of the Achilles tendon such as tendonitis or bursitis, Achilles tendon rupture is usually treated with surgical repair. The surgery consists of making a small incision in the back part of the leg, and using sutures to re-attach the two ends of the ruptured tendon. Depending on the condition of the ends of the ruptured tendon and the amount of separation, the surgeon may use other tendons to reinforce the repair. After the surgery, the leg will be immobilized for 6-8 weeks in a walking boot, cast, brace, or splint. Following this time period, patients work with a physical therapist to gradually regain their range of motion and strength. Return to full activity can take quite a long time, usually between 6 months and 1 year.
Surgical Treatment Unlike other diseases of the Achilles tendon such as tendonitis or bursitis, Achilles tendon rupture is usually treated with surgical repair. The surgery consists of making a small incision in the back part of the leg, and using sutures to re-attach the two ends of the ruptured tendon. Depending on the condition of the ends of the ruptured tendon and the amount of separation, the surgeon may use other tendons to reinforce the repair. After the surgery, the leg will be immobilized for 6-8 weeks in a walking boot, cast, brace, or splint. Following this time period, patients work with a physical therapist to gradually regain their range of motion and strength. Return to full activity can take quite a long time, usually between 6 months and 1 year.
 Achilles tendon ruptures may be divided into full thickness ("total") and partial thickness ruptures. Total ruptures usually occur in formerly active athletes (average age 40) who resume sport activity after having been away from it for some time. In these cases, degenerative changes have weakened the tendon so much that sudden, forceful loading of the tendon causes it to tear. To some extent, these changes in the tendon could have been prevented by regular physical activity. In most cases, the injury
Achilles tendon ruptures may be divided into full thickness ("total") and partial thickness ruptures. Total ruptures usually occur in formerly active athletes (average age 40) who resume sport activity after having been away from it for some time. In these cases, degenerative changes have weakened the tendon so much that sudden, forceful loading of the tendon causes it to tear. To some extent, these changes in the tendon could have been prevented by regular physical activity. In most cases, the injury
